Related guidance: Gout: diagnosis and management NICE guideline (NG219 June 2022)
- Suspect gout when presented with rapid onset of severe pain together with redness and swelling, in one or both first metatarsophalangeal (MTP) joints and tophi. Consider gout in joints other than the first MTP joints (for example, midfoot, ankle, knee, hand, wrist, elbow).
- Assess the possibility of septic arthritis, calcium pyrophosphate crystal deposition and inflammatory arthritis when presented with a painful, red, swollen joint. Consider chronic gouty arthritis when presented with chronic inflammatory joint pain.
- Measure the serum urate level to confirm the clinical diagnosis of gout (serum urate level of 360 umol/L or more). If serum urate level is below 360 umol/L during a flare and gout is strongly suspected, repeat the serum urate level measurement at least 2 weeks after the flare has settled. Consider joint aspiration and microscopy of synovial fluid if a diagnosis of gout remains uncertain or unconfirmed. If joint aspiration cannot be carried out or the diagnosis of gout remains uncertain, consider imaging the affected joints with X-ray, ultrasound or dual-energy CT.
- Offer a non-steroidal anti-inflammatory drug (NSAID), colchicine or a short course of an oral corticosteroid for first-line treatment of a gout flare, considering the person’s comorbidities, co-prescriptions and preferences. See oral NSAIDs and Corticosteriods in formulary.
- Applying ice packs to the affected joint (cold therapy) in addition to taking prescribed medicine may help alleviate pain.
- Consider an intra-articular or intramuscular corticosteroid injection to treat a gout flare if NSAIDs and colchicine are contraindicated, not tolerated or ineffective. See injectable Corticosteriods in formulary.
- Refer the person to a rheumatology if NSAIDs, colchicine and corticosteroids are contraindicated, not tolerated or ineffective.
- Consider a follow-up appointment after a gout flare has settled to measure the serum urate level, provide information about gout and how to self-manage and reduce the risk of future flares, assess lifestyle and comorbidities (including cardiovascular risk factors and CKD), review medications and discuss the risks and benefits of long-term ULT (urate-lowering therapies).VersusArthritis gout patient information booklet
- There is not enough evidence to show that any specific diet prevents flares or lowers serum urate levels. Advise a healthy, balanced diet. Excess body weight or obesity and excessive alcohol consumption may exacerbate gout flares and symptoms.
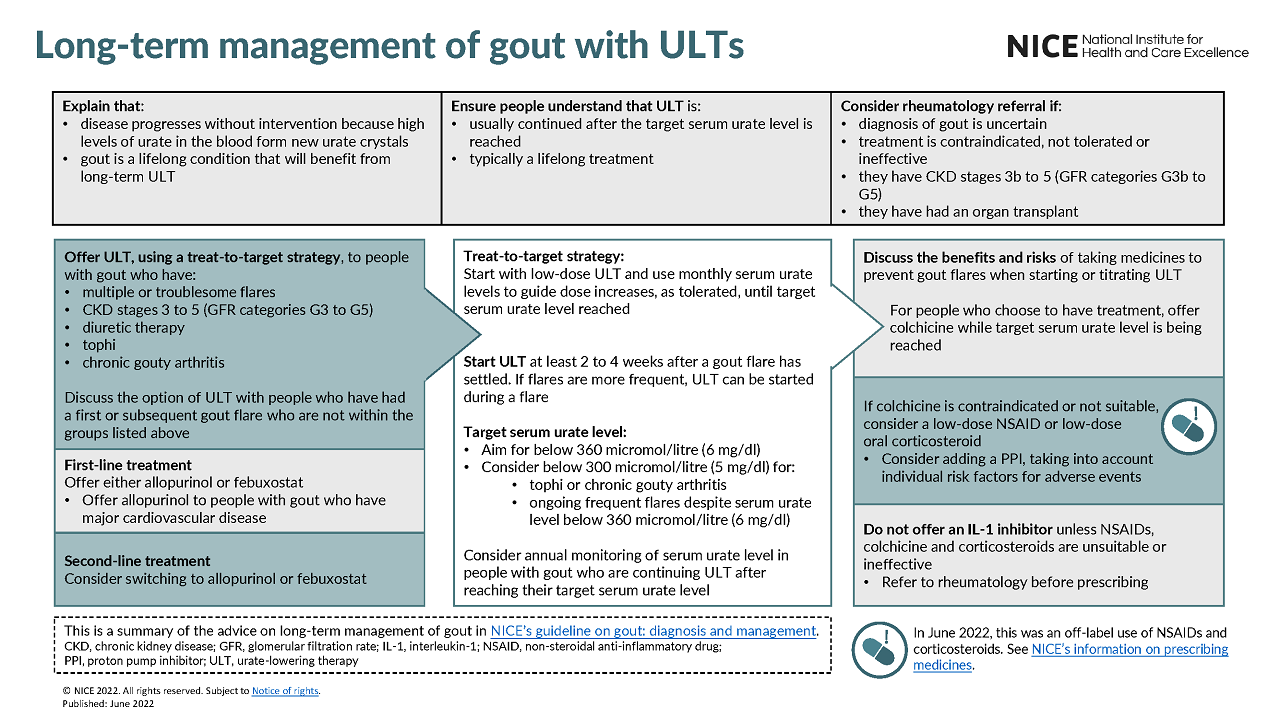
- Offer ULT starting with a low dose and use monthly serum urate levels to guide dose increases, as tolerated, until the target serum urate level is reached (treat-to-target strategy) in people with gout who have multiple or troublesome flares, CKD stages 3 to 5, diuretic therapy, tophi, and chronic gouty arthritis.
- Discuss the option of ULT, using a treat-to-target strategy, with people who have had a first or subsequent gout flare.
- Ensure people understand that ULT is usually continued after the target serum urate level is reached and is typically a lifelong treatment.
- Start ULT at least 2 to 4 weeks after a gout flare has settled. If flares are more frequent, ULT can be started during a flare.
- Aim for a target serum urate level below 360 umol/L. Consider a lower target serum urate level below 300 umol/L for people with gout who have tophi or chronic gouty arthritis or continue to have ongoing frequent flares despite having a serum urate level below 360 umol/L.
- Offer either allopurinol or febuxostat as first-line treatment when starting treat-to-target ULT, considering the person’s comorbidities and preferences. Offer allopurinol as first-line treatment to people with gout who have major cardiovascular disease (for example, previous myocardial infarction or stroke, or unstable angina). Consider switching to second-line treatment with allopurinol or febuxostat if the target serum urate level is not reached or first-line treatment is not tolerated.
- Discuss the benefits and risks of taking medicines to prevent gout flares when starting or titrating ULT. For people who choose to have treatment to prevent gout flares when starting or titrating ULT, offer colchicine while the target serum urate level is being reached. If colchicine is contraindicated, not tolerated or ineffective, consider a low-dose NSAID or low-dose oral corticosteroid. See oral NSAID’s and Corticosteriods in formulary.
NICE recommends a proton pump inhibitor (PPI) is co-prescribed when offering treatment with an oral NSAID or COX-2 inhibitor NSAID. See Gastric acid disorders and ulceration in formulary.
- Use oral NSAIDs or COX-2 inhibitor NSAIDs at the lowest effective dose for the shortest possible period of time.
- All oral NSAIDs or COX-2 inhibitor NSAIDs have analgesic effects of a similar magnitude but vary in their potential gastrointestinal, liver and cardio-renal toxicity; therefore, when choosing the agent and dose, take into account individual patient risk factors, including age and consideration should be given to appropriate assessment and/or ongoing monitoring of these risk factors.
NICE recommends bone protection treatment should be considered in people taking high doses of glucocorticoids (prednisolone ≥7.5 mg daily or equivalent) for 3 months or longer. See Disorders of bone metabolism in formulary.
NHS Somerset recommends Losartan as the first choice for people with a history of gout and cardiac comorbidity who need an Angiotensin-converting enzyme inhibitor or Angiotensin II Receptor Blocker;
Losartan demonstrated statistically significant reductions in serum uric acid levels or increases in fractional excretion of uric acid in all studies, whereas no other ARB reached statistical benefit. The effect of ARBs on the occurrence of gout attacks or other clinical outcomes were not represented. Four studies evaluated safety effects of these agents indicating abnormalities such as minor changes in lab values. In conclusion, losartan is the only ARB that has consistently demonstrated a significant reduction in serum uric acid levels, although the significance of impacting clinical outcomes remains unknown. Losartan appears to be a safe and efficacious agent to lower serum uric acid levels in patients with hyperuricemia.See The effect of angiotensin II receptor blockers on hyperuricemia. Therapeutic Advances in Chronic Disease (2015).See ARBs in formulary.
NICE Gout Clinical Knowledge Summary (updated June 2022)
| Therapeutic Area | Formulary Choices | Cost for 28 (unless otherwise stated) | Rationale for decision / comments |
|---|---|---|---|
| Treatment for gout flares | |||
| Colchicine | 500mcg tablets: £3.42 (100) | ||
| Long-term management of gout | |||
| First-line | Allopurinol | 100mg tablets: £0.79 300mg tablets: £1.12 | |
| Febuxostat | 80mg tablets: £2.44 (28) 120mg tablets: £24.36 (28) | Febuxostat: increased risk of cardiovascular death and all-cause mortality in clinical trial in patients with a history of major cardiovascular disease MHRA Drug Safety Update | |
| Sulfinpyrazone is unlicensed, refer to specialist. | |||
Figure 1 Management of gout

Figure 2 Long-term management of gout with ULTs