
Related guidance:
![]()
Initial assessment
- Healthcare professionals should consider assessment for irritable bowel syndrome (IBS) if the person reports having had any of the following symptoms for at least 6 months:
- Abdominal pain or discomfort
- Bloating
- Change in bowel habit. - A diagnosis of IBS should be considered only if the person has abdominal pain or discomfort that is either relieved by defaecation or associated with altered bowel frequency or stool form. This should be accompanied by at least 2 of the following 4 symptoms:
- altered stool passage (straining, urgency, incomplete evacuation)
- abdominal bloating (more common in women than men), distension, tension or hardness
- symptoms made worse by eating
- passage of mucus.
Other features such as lethargy, nausea, backache and bladder symptoms are common in people with IBS, and may be used to support the diagnosis.
Diagnostic tests
- In people who meet the IBS diagnostic criteria, the following tests should be undertaken to exclude other diagnoses:
- full blood count (FBC)
- erythrocyte sedimentation rate (ESR) or plasma viscosity
- c-reactive protein (CRP)
- antibody testing for coeliac disease (endomysial antibodies [EMA] or tissue transglutaminase [TTG]).
• The following tests are not necessary to confirm diagnosis in people who meet the IBS diagnostic criteria:
- ultrasound
- rigid/flexible sigmoidoscopy
- colonoscopy; barium enema
- thyroid function test
- faecal ova and parasite test
- faecal occult blood
- hydrogen breath test (for lactose intolerance and bacterial overgrowth).
Dietary and lifestyle advice
- People with IBS should be given information that explains the importance of self-help in effectively managing their IBS. This should include information on general lifestyle, physical activity, diet and symptom-targeted medication.
- Healthcare professionals should review the fibre intake of people with IBS, adjusting (usually reducing) it while monitoring the effect on symptoms. People with IBS should be discouraged from eating insoluble fibre (for example, bran). If an increase in dietary fibre is advised, it should be soluble fibre such as ispaghula powder or foods high in soluble fibre (for example, oats).

Irritable bowel syndrome and diet factsheet (BDA)
Pharmacological therapy
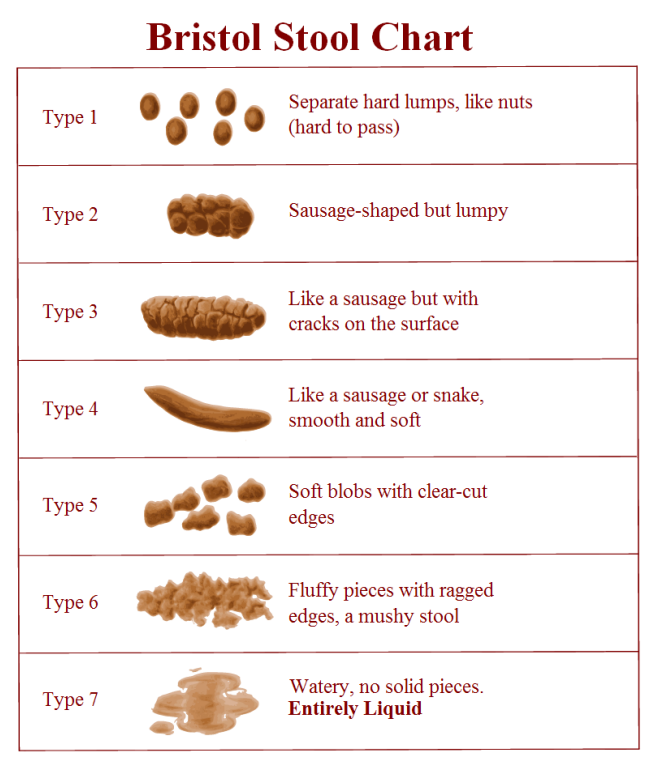
- People with IBS should be advised how to adjust their doses of laxative or antimotility agent according to the clinical response. The dose should be titrated according to stool consistency, with the aim of achieving a soft, well-formed stool (corresponding to Bristol Stool Form Scale type 4).
- Consider tricyclic antidepressants (TCAs) as second-line treatment for people with IBS if laxatives, loperamide or antispasmodics have not helped. Start treatment at a low dose, 5 mg to 10 mg of amitriptyline, taken once at night, and review regularly. Increase the dose if needed, but not usually beyond 30 mg.
For laxatives see NHS Somerset Formulary Constipation and bowel cleansing disorders
For loperamide see NHS Somerset Formulary Diarrhoea
For amitriptyline see NHS Somerset Formulary Depression
Irritable bowel syndrome: Antispasmodic drugs (NICE CKS September 2022)
| Therapeutic Area | Formulary Choices | Cost for 28 (unless otherwise stated) | Rationale for decision / comments |
|---|---|---|---|
| Antispasmodics | Mebeverine | 135mg tablet: £3.29 (100) | One tablet three times a day, dose preferably taken 20 minutes before meals. Avoid prescribing as Colofac IBS as this is not cost effective. |
| Peppermint oil as | 0.2ml gastro-resistant capsule: £7.04 (84) | One to two capsules taken three times a day for up to 2–3 months if needed, dose to be taken before meals, swallowed whole with water. | |
| Antimuscarinics | Hyoscine butylbromide | 10mg tablet: £3.83 (56) | For symptomatic relief of gastro-intestinal disorders characterised by smooth muscle spasm. Child 12-17 years and Adult: 20 mg 4 times a day. For irritable bowel syndrome. Adult: 10 mg 3 times a day; increased if necessary up to 20 mg 4 times a day. |
| 20mg/1ml solution for injection ampoule: £3.89 (10) | For palliative care as per Wessex palliative care handbook. | ||
| Propantheline bromide | 15mg tablet: £20.74 (112) | For symptomatic relief of gastro-intestinal disorders characterised by smooth muscle spasm. Adult: 15 mg 3 times a day, dose to be taken at least one hour before food and 30 mg, dose to be taken at bedtime; maximum 120 mg per day. |
|
| NHS Somerset classify Dicycloverine as non-formulary as not cost effective. | |||