
Related guidance:
![]()
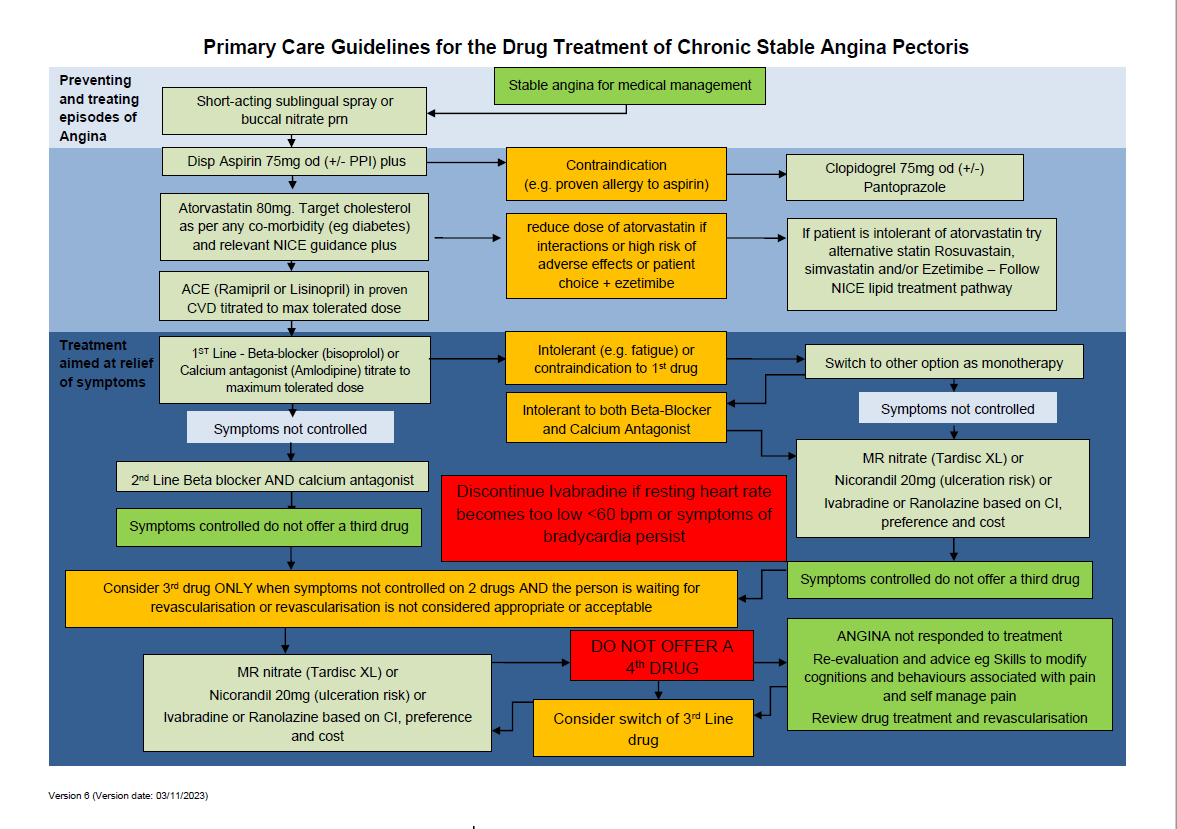
Acute coronary syndromes NICE guideline (NG185 November 2020)
Stable angina: management Clinical guideline (CG126 July 2011, updated August 2016)

| Therapeutic Area | Formulary Choices | Cost for 28 (unless otherwise stated) | Rationale for decision / comments |
|---|---|---|---|
| Nitrates | Glyceryl trinitrate | 400micrograms/dose pump sublingual spray: £2.27 (180 dose), £2.48 (200 dose) | For treatment of angina. Glyceryl trinitrate tablets are significantly more costly than spray and will need to be discarded 8 weeks after opening. The aerosol spray is twice the price of the pump spray. 400-800 mcg, to be administered under the tongue, when sitting down. Dose may be repeated at 5-minute intervals if required. If symptoms have not resolved after 3 doses, medical attention must be sought. |
| Isosorbide mononitrate | 10mg tablet: £0.96 (56) | For angina prophylaxis. Adult: initially 10 mg twice daily, increased if necessary up to 120 mg daily in divided doses. Where Isosorbide mononitrate has been added to provide symptom control pending angioplasty or CABG, consideration should be given to cautious withdrawal after successful completion of and recovery from the procedure. The second of the two daily immediate release doses should be given after about 8 hours rather than 12 hours to maintain nitrate free period to avoid tolerance developing with reduced therapeutic effect. |
|
| 20mg: £1.19 (56) | |||
| 40mg: £1.35 (56) | |||
| as Tardisc XL® | 60mg modified-release tablet: £3.49 | Adult: initially half a tablet daily for 2–4 days, to minimise possibility of headache, then 1 tablet daily, increased if necessary to 2 tablets daily, dose to be taken in the morning. Modified release formulations should only be given once daily to maintain nitrate free period to avoid tolerance developing with reduced therapeutic effect. |
|
| as Monomil XL® | 60mg modified-release tablet: £3.49 | ||
| as Chemydur XL® | 60mg modified-release tablet: £3.49 | ||
| Isosorbide dinitrate is Non-formulary except when initiated by a specialist for left ventricular failure. | |||
| Vasodilators, Potassium-channel openers | Nicorandil | 10mg tablet: £1.71 (60) | For angina prophylaxis. Adult: initially 5–10 mg twice daily, then increased if tolerated to 40 mg twice daily; usual dose 10–20 mg twice daily, use lower initial dose regimen if patient susceptible to headache. Where Nicorandil has been added for symptom control pending angioplasty or CABG, consideration should be given to cautious withdrawal after successful completion of and recovery from the procedure. Nicorandil is associated with oral, anal, gastro-intestinal, para-stomal ulceration & delayed wound healing. Addition of a PPI is ineffective to promote healing – cessation of the drug is needed. |
| 20mg tablet: £2.17 (60) | |||
| Updated advice on use of nicorandil as second-line treatment for stable angina - some ulcers may progress to complications unless treatment is stopped. See MHRA (January 2016) for Nicorandil (Ikorel): now second-line treatment for angina - risk of ulcer complications. | |||
| Selective sinus node IF inhibitor | Ivabradine | 5mg tablet: £28.25 (56) | For treatment of angina. Adult: (18–74 years) initially 2.5–5 mg twice daily for 3–4 weeks, then increased if necessary up to 7.5 mg twice daily, dose to be increased gradually; reduced if not tolerated to 2.5–5 mg twice daily, heart rate at rest should not be allowed to fall below 50 beats per minute, discontinue treatment if no improvement in symptoms within 3 months. Adult: (75 years and over) initially 2.5 mg twice daily for 3–4 weeks, then increased if necessary up to 7.5 mg twice daily, dose to be increased gradually; reduced if not tolerated to 2.5–5 mg twice daily, heart rate at rest should not be allowed to fall below 50 beats per minute, discontinue treatment if no improvement in symptoms within 3 months. For treatment of chronic heart failure. Adult: (18–74 years) initially 5 mg twice daily for 2 weeks, then increased if necessary to 7.5 mg twice daily; reduced if not tolerated to 2.5–5 mg twice daily, heart rate at rest should not be allowed to fall below 50 beats per minute. Adult: (75 years and over) initially 2.5 mg twice daily for 2 weeks, then increased if necessary up to 7.5 mg twice daily, dose to be increased gradually; reduced if not tolerated to 2.5–5 mg twice daily, heart rate at rest should not be allowed to fall below 50 beats per minute. QT prolongation may be exacerbated by heart rate reduction. The use of ivabradine with other drugs which prolong QT interval such as citalopram and diltiazem should be avoided. If the combination is necessary, close cardiac monitoring is needed. Hypokalaemia and hypomagnesaemia can increase the risk of arrhythmia especially in patients with long QT interval, whether congenital or substance-induced for example with potassium-depleting diuretics (thiazide diuretics and loop diuretics). Caution & careful monitoring is needed. |
| 7.5mg tablet: £31.33 (56) | |||
| Piperazine derivatives | Ranolazine | 375mg modified-release tablet: £48.98 (60) | Treatment of stable angina. Adult: initially 375 mg twice daily for 2–4 weeks, then increased to 500 mg twice daily, then adjusted according to response to 750 mg twice daily; reduced if not tolerated to 375–500 mg twice daily. |
| 500mg modified-release tablet: £48.98 (60) | |||
| 750mg modified-release tablet: £48.98 (60) | |||